In 2004 President George W. Bush suggested that all Americans should have have an electronic health record (EHR) by the year 2014.
A key component of these EHRs was the improvement of medication management.
In 2006 the Healthcare Information Management and Systems Society (HIMSS) Analytics began tracking the rate of adoption of EHR mechanisms in hospitals. They found that only 3.6% of hospitals had computerized provider order entry (CPOE) and electronic medication administration records (EMARs).
Electronic health records can be implemented in a variety of ways, provide many different functions, and achieved a multiplicity of purposes. In 2008, the federal government requested the development of definitive definitions for electronic health records.
These definitions are:
- Electronic medical record – an electronic record of health-related information on an individual that can be created, gathered, managed, and consulted by authorized clinicians and staff within one healthcare organization.
- Electronic health record – an electronic record of health-related information on an individual that conforms to nationally recognized interoperability standards and that can be created, managed, and consulted by authorized clinicians and staff across more than one healthcare organization.
In 2008, HIMSS Analytics found an increase of only 5.8% of hospitals using the applications. Therefore, in 2009 President Barack Obama incorporated incentives for hospitals and physicians to make meaningful use of certified EHR technology into his legislation (the American Recovery and Reinvestment Act [ARRA] of 2009 and Health Information Technology for Economic and Clinical Health Act [HITECH]. This incentive program is referred to simply as meaningful use (M.U.).
In 2010, the federal government published regulations that illustrated prerequisites to receiving incentives for M.U. of certified EHR technology. They implemented the term EHR, but also added a definition of qualified EHR (45 CFR 170 Subpart B):
A qualified EHR is an electronic record of health-related information on an individual that –
1. includes patient demographic and clinical health information, such as medical history and problem list, and
2. has the capacity to –
a. provide clinical decision support;
b. support physician order entry;
c. capture and query information relevant to healthcare quality; and
d. exchange electronic health information with and integrate such
information from other sources (ARRA 2009).
By 2012, HIMSS Analytics acknowledged that 25% of hospitals had adopted CPOE systems and other essential EHR tools. HIMSS Analytics also began tracking ambulatory care facilities for their implementations of EHRs in 2012 and estimated that fewer than half of physicians used any form of automation. But when using automation, the majority were at least basic EHR systems (HIMSS Analytics 2012).
Certified EHR Technology (CEHRT) is the name used to describe EHR products meeting specified standards and criteria. The M.U. criteria integrated stronger functionality than typically employed in the past but excluded some functionality necessary for implementation of EHRs.
The federal government acknowledged functionality issues in two ways:
1. they permitted EHR products to have one of two certifications-
complete: all functionality that would enable users to earn the M.U. incentives were included, or
modular: only certain functionality was included in the product. To be able to earn incentives the organization had to use a set of modular products that, together, address all required criteria.
2. they observed that the M.U. certification criteria represented the minimum capabilities EHR technology needed to include and have properly implemented to achieve certification for the purposes of earning incentives and that these criteria do not preclude complete EHR vendors from including additional capabilities not required for certification (Federal Register 2010, 44595).
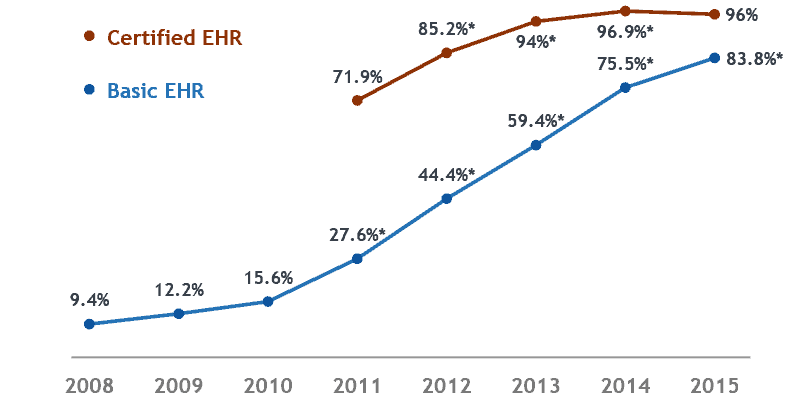
A data brief made available on the HealthIT.gov Dashboard showed hospital adoption of basic EHR technology rose from 75.5% in 2014 to 83.8% in 2015 but put the percentage of hospitals with CEHRT at 96% in 2015, down nearly a full percentage point from 2014’s figure of 96.9%.
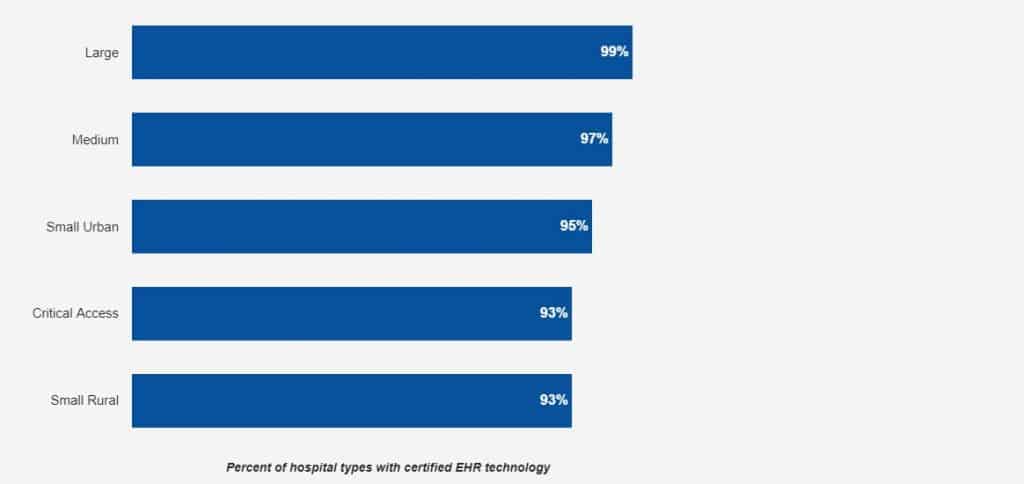
In 2017, 96 percent of all non-federal acute care hospitals possessed certified health IT. Small rural and critical access hospitals had the lowest rates at 93 percent. Ninety-nine percent of large hospitals (more than 300 beds) had certified health IT, while 97 percent of medium-sized hospitals (more than 100 beds) had certified health IT.
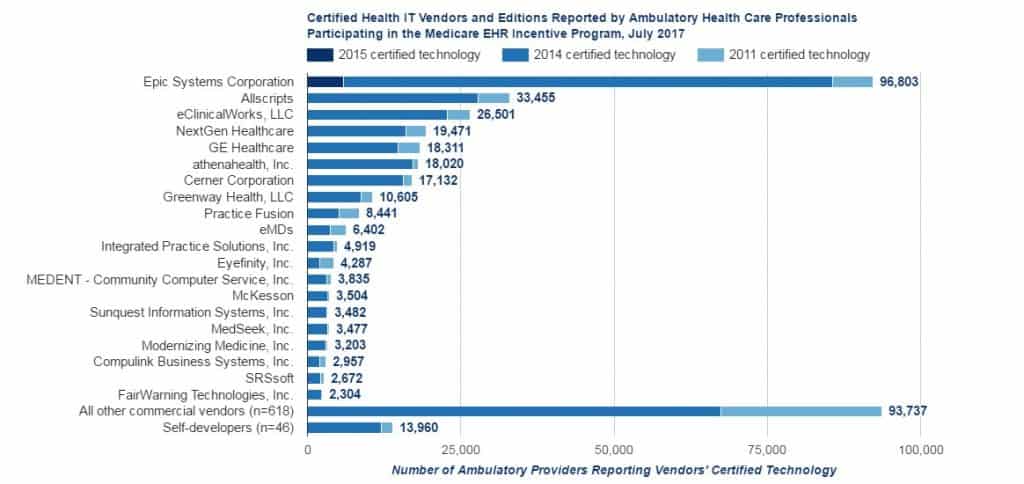
As of July 2017, 684 health IT developers supply certified health IT to 354,395 ambulatory primary care physicians, medical and surgical specialists, podiatrists, optometrists, dentists, and chiropractors participating in the Medicare EHR Incentive Program.
Of those 354,395 providers, over 82% have 2014 certified edition technology. Epic Systems, Allscripts, eClinicalWorks, athenahealth, and NextGen Healthcare supply 2014 certified technology to 60% of all providers that have reported 2014 edition technology. Epic Systems, alone, supplies 2014 certified technology to over 30% of all those providers.
Adoption of EHR systems has steadily increased since HITECH. Basic EHR adoption represents a minimum use of core functionality determined to be essential to an EHR system. Moreover, since the passage of the HITECH Act in 2009, state EHR adoption rates have increased.
In addition to growth in EHR adoption overall, hospital adoption of technology with advanced functionality increased significantly. While fewer hospitals used Basic EHR systems without clinician notes, significantly more adopted systems with clinician notes.
Finally, a vast majority of acute care hospitals (97%) possess EHR technology certified to meet federal requirements. These hospitals should have the technology needed to meet EHR Incentive Program objectives.
These systems are also certified to be secure and able to work with other certified systems to share information. Thus, the increase in the rate of adoption for certified EHR technology shed a positive light on hospitals’ progress towards the interoperable exchange of health information.
If you are an attorney, please contact Krug Consulting to assist with all of your cases involving EHRs.
Click to call us at 1 (844) LNC-KRUG • or Contact Us via email
Our Legal Nurse Consultants will review all the relevant documents, prepare reports, research injuries and locate experts for plaintiff or defense.
If you find this blog helpful, please share it with colleagues, or direct them to our website.
References and Resources
45 CFR 170 Subpart B. 2010 (July 28). Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, Final Rule.
Federal Register, 2010 (July 28). 45 CFR 170: Health Information Technology: Initial Set of Standards, Implementation Specifications, and Certification Criteria for EHR Technology; Final Rule, p. 44595.
Healthcare Information Management and Systems Society. 2006-2013. HIMSS Analytics US EMR Adoption Model. Chicago, IL:HIMSS.
National Alliance for Health Information Technology. 2008 (April 28). Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms.


